A Disease-Modifying Approach to Wet AMD, Geographic Atrophy, and Diabetic Retinopathy
Phase IIa complete. First-in-class CXCR3 agonist with clinically demonstrated anti-fibrotic, anti-angiogenic, and disease-modifying activity
Welcome to
OCUGENIX
Ocugenix has programs in three ocular indications that have just completed Phase I studies:
1
Wet Macular Degeneration
2
Geographic
Atrophy
3
Proliferative Diabetic Retinopathy
The company has initiated a Phase II program for wet macular degeneration and anticipates reporting preliminary results by the end of 2025.
Ocugenix has an additional ocular indication in Dry Eye, which is in the IND-enabling stage.
Patients Dosed
Phase I and Phase IIa clinical experience with no compound-related safety issues
IRF/SRF Resolution
Intraretinal and subretinal fluid cleared in >80% of evaluable patients, vs. ~50% with Vabysmo
SHRM Resolution
Fibrosis biomarker eliminated in >80% of patients, vs. 28–30% for anti-VEGF agents
Months Disease-Free
Patients maintained visual acuity and retinal stability for 6+ months after the last injection
How We Are
DIFFERENT
Ocugenix is the only company in ophthalmology that seeks to harness the body’s natural wound-healing processes to restore homeostatic functioning in the eye.
Our agonists activate signaling pathways that counter chronic inflammation and promote regenerative repair. Other drugs in these target indications inhibit specific symptoms of their disease, such as the edema that is the result of leakage in the pathological vessels. By targeting a single symptom or disease process, such as VEGF or complement, approaches are limited because these diseases are multifactorial. Our therapies are disease-modifying by pharmacologically coopting the entire physiologic cascade that restores homeostasis.
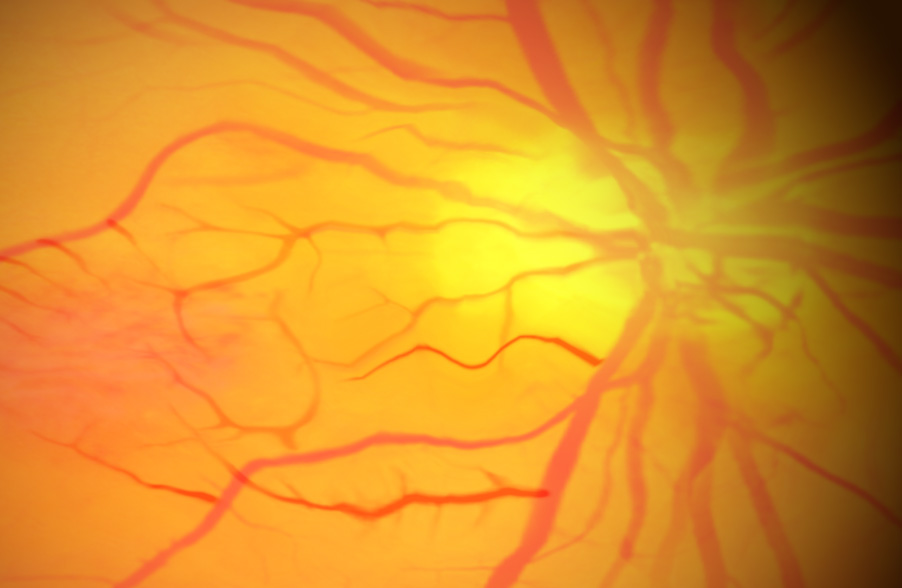
Wet AMD
Our initial target indication, wet AMD, reflects this difference in approach. Current anti-VEGF therapies counter the excessive amounts of VEGF, causing the aberrant blood vessels to constrict, thus reducing the edema, the cause of the initial symptoms of wet AMD. Unfortunately, these anti-VEGF agents do nothing to eliminate these pathological blood vessels and do nothing to reduce the development of fibrosis, which is the cause of long-term blindness that all wet AMD patients will ultimately develop. Only OGX-110 activates the processes that shut down and remove the pathological vessels and fibrosis formation.
Geographic Atrophy
- In Geographic Atrophy, complement cascade inhibitors slow the rate of growth of the geographic lesion by about 25%. Unfortunately, many other factors outside of the complement system contribute to this lesion growth, and these factors remain active even when the complement system is blocked.
- Only OGX-110 shuts down the chronic wound response to initiate resolution, blunting the effect of all inflammatory factors and other stimulants of lesion growth.
Dry Eye
- In Dry Eye, inflammation on the surface of the eye (caused by a variety of factors) results in significant discomfort to the patient.
- Only OGX-110 has shown the ability to end the inflammation and support the regeneration of the stem cells. It has the unique ability to shut down the disease at its source and restore a healthy micro-environment.
- This activity has been demonstrated in extensive animal studies.
- Only OGX-110 activates the processes that shut down and remove the pathological vessels and fibrosis formation.
- In Geographic Atrophy, complement cascade inhibitors slow the growth of the geographic lesion by about 25%. Unfortunately, many other factors outside of the complement system contribute to this lesion growth, and these factors remain in effect even when the complement system is blocked.
- Only OGX-110 shuts down the chronic wound to initiate resolution, blunting the effect of all inflammatory factors and other stimulants of lesion growth.
- In Dry Eye, inflammation on the surface of the eye (caused by various factors) results in significant discomfort to the patient.
- Only OGX-110 has shown the ability to end the inflammation and support the regeneration of the stem cells. It has the unique ability to shut down the disease at its source and restore a healthy micro-environment.
Our Target Indications
Wet Macular Degeneration
About 200,000 new cases of wet AMD are diagnosed each year in North America. Due to the aging population, the National Eye Institute estimates that the prevalence of advanced AMD will grow to 5 million by 2040.
In wet AMD, an aberrant wound response leads to the proliferation of blood vessels and a fibrotic growth starting in the macula, the area of the retina responsible for central vision. Damage to photoreceptors in the macula can cause distortion or blind spots in a person’s central vision. Patients with wet AMD who are untreated or for whom treatment is ineffective (about 30% to 50%) can progress to total blindness. VEGF inhibitors address the edema released by this pathological vasculature in most patients, with most of these becoming less responsive over time; thus, there is a need for other mechanisms to reduce the edema. More importantly, the anti-VEGF therapies do nothing to cause the regression of the pathological vessels or limit the fibrosis responsible for the long-term loss of sight. This is an unmet clinical need not addressed by any other compounds in development for AMD.
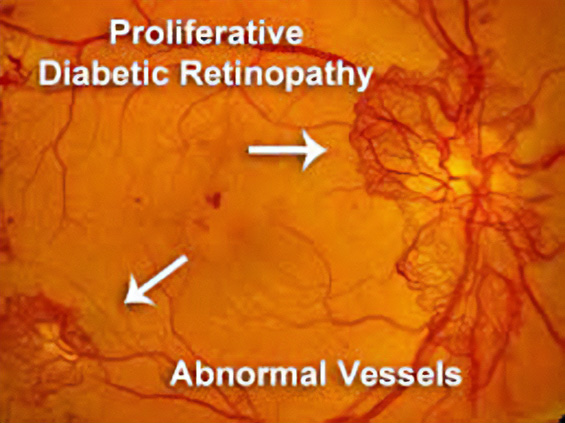
In 2021, across all ages, an estimated 9.6 million people in the United States were living with diabetic retinopathy (DR). Of these, 1.84 million were living with vision-threatening proliferative DR (pDR) or late-stage Diabetic Retinopathy. In diabetic retinopathy, abnormal, “leaky” blood vessels release fluid and can cause hemorrhages. At the advanced stage of the disease, new vessels infiltrate the retina, leading to the formation of fibrotic tissue on the retinal surface or in the vitreous cavity, vitreous hemorrhage, retinal detachment, retinal damage, and loss of vision.
These blood vessels, which are thin, weak, and prone to bleeding, cause scar tissue to form inside the eye. This scar tissue can pull the retina away from the back of your eye, causing retinal detachment. A detached retina typically results in blurriness, a reduced field of vision, and, in severe cases, permanent loss of vision. Laser photocoagulation is often effective; however, the procedure can be painful and may result in loss of peripheral vision. Anti-VEGF therapies are effective for a large percentage of patients, but as many as 25% do not respond even at the start, and many more become resistant over time.
OGX-110 has been shown to cause the regression of these nascent pathologic vessels in the animal model of pDR and to suppress the development of fibrosis. This novel mechanism of action holds great promise for improving sight in the short term and ultimately shutting down the drivers of the disease.
Geographic Atrophy
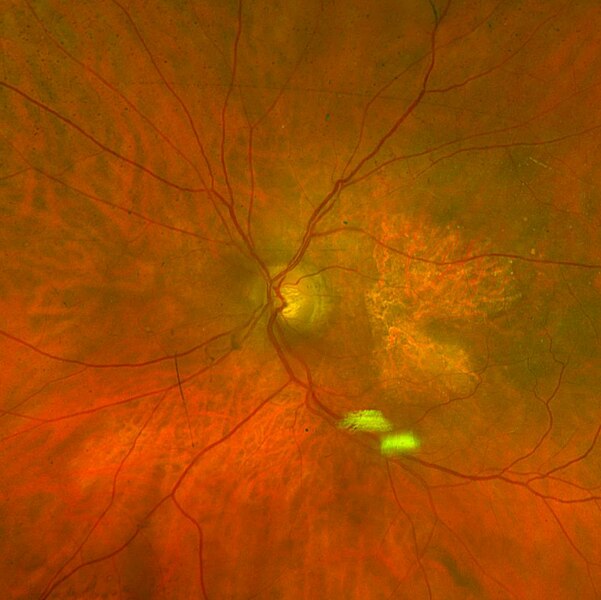
More than 5 million people worldwide have geographic atrophy, including nearly 1 million in the U.S. In developed nations, approximately 1 in 29 people over the age of 75 have geographic atrophy, which increases to almost 1 in 4 people over the age of 90.
With aging, the retinal pigment epithelium (RPE) is exposed to intrinsic and extrinsic oxidative and environmental stressors such as cigarette smoke. The cytotoxic damage accumulates, resulting in the formation of drusen, yellow deposits of lipids between the RPE and Bruch’s membrane. Excessive drusen accumulation and drusen components, such as cellular debris, lipids, and lipoproteins, may trigger chronic inflammation through multiple pathways, including a chronic wound response. Chronic inflammation, a result of the wound response, can eventually lead to photoreceptor, RPE, and choriocapillaris cell death, causing the appearance of sharply defined atrophic lesions that are characteristic of GA and the appearance of choroidal vessels due to the missing RPE layer.
Two therapies limiting different aspects of the complement cascade were recently approved as the first agents to treat GA. Unfortunately, each of these agents reduces the growth rate of the lesions by only about one-quarter and, therefore, does not significantly impact the retention of visual acuity, at least within the first year or two. This continued progression of the disease demonstrates a gap in treatments and argues for new mechanisms by which to shut down the chronic wound response that leads to GA.
By activating the CXCR3 pathway, OGX-110 triggers an irreversible molecular cascade that resolves the wound response, suppressing inflammation, the development of fibrosis, and the regression of the choroidal vessels.
Dry Eye
Approximately 39 million patients in the United States suffer from Dry Eye Disease (DED). Symptoms include ocular pain, dryness, and a persistent, gritty sensation, which are all too familiar persistent aspects of the disease. DED can be secondary to many insults, the major ones being dry or salty air, air pollution, surgical damage of the ocular surface, and viral and autoimmune diseases. The commonality of all these causes is that a loss of tears eventually damages the goblet cells that produce the mucin that binds the tears to the eye’s surface.
There are presently five FDA-approved therapeutics for the treatment of dry eye disease. The first one, Restasis, was approved twenty years ago, but the pace of approvals has picked up significantly in the last three years. While most approved therapies focus on limiting the autoimmune activation that can lead to DED, the vast majority of DED is caused by environmental, chemical, and surgical insults. This singular focus on immune-driven DED is one of the main reasons that existing drugs have such marginal benefits.
Significant unmet clinical needs remain. The largest of these are treatments that can impact the goblet cells, the origin of mucin, and meibomian gland dysfunction (MGD), the source of the lipid layer in tears. Our animal studies demonstrate that our therapy, which causes the regeneration of goblet cells, can positively affect environmental, surgical, and chemical-based DED. As the goblet cell functioning is central to DED, and we have found that our agent can restore this function, Ocugenix is uniquely positioned to be disease-modifying in DED.